- Research
- Open access
- Published:
Chronic diseases and catastrophic health expenditures in elderly Chinese households: a cohort study
BMC Geriatrics volume 25, Article number: 272 (2025)
Abstract
Background
Catastrophic health expenditure (CHE) is a key indicator for studying the economic burden of diseases. Previous study mainly focused on exploring the relationship between severe diseases such as cancer and multimorbidity with CHE. However, there is a lack of research exploring the differential effects of single and multiple chronic diseases on CHE. This study aims to analyse the longitudinal association between different chronic disease conditions and CHE among elderly households in China, and investigate whether this association is influenced by other demographic and socioeconomic variables.
Methods
A total of 6,483 older adults obtained from four waves (2013, 2015, 2018, 2020) of the China Health and Retirement Longitudinal Study (CHARLS) were analysed (elderly household without CHE at baseline were included). CHE was defined as out-of-pocket health expenditures exceeding 40% of household non-food expenditures. Mixed-effects logistic regression models were employed to explore the longitudinal relationship between different chronic diseases conditions and CHE, and stratification analyses were conducted to explore the potential moderation effect.
Result
The analysis indicates that both single chronic diseases(P < 0.001) and multimorbidity(P < 0.001) significantly increase the risk of CHE in elderly households. A stratified analysis based on population and socio-economic variables showed similar results. Besides, when the threshold for CHE was set at 40% of household non-food expenditures, the risk increase for CHE was similar for both elderly individuals with single and multiple chronic diseases. However, when the threshold was lowered to 10%, 25% of total household expenditures or 25% of household non-food expenditures, elderly individuals with multiple chronic diseases had a higher risk of CHE compared to those with a single chronic disease or without chronic disease. The influencing factors of CHE included age, education level, marital status, hukou, and place of residence. In particular, basic medical insurance did not significantly reduce the risk of CHE.
Conclusion
Both single and multiple chronic diseases significantly increase the risk of catastrophic health expenditure among elderly households in China, and the existing basic medical insurance coverage has not effectively alleviated this burden. The findings highlight the urgent need for improving social health insurance programs, as well as conducting differentiated financial protection strategies for elderly individuals with different chronic disease statuses to reduce the financial vulnerability of elderly households with chronic diseases.
Background
Each year, 44 million households worldwide encounter catastrophic health expenditures (CHE), especially in low and middle-income countries with inadequate healthcare systems [1]. CHE occurs when a family’s healthcare costs surpass a significant portion of their income, which will severely affect their well-being, increase the risk of poverty, and thereby widen the gap between the wealthy and vulnerable groups [2]. In China, the prevalence of such financially ruinous health costs is on the rise among households.
In recent years, chronic diseases have become a significant public health problem impacting China’s economic and social development. Meanwhile, chronic conditions are major contributors to the health burden, health outcome inequalities, and economic strain. The proportion of deaths caused by chronic diseases in China increased from 80.0% in 2002 to 86.6% in 2012 and 88.5% in 2018 [3]. If no effective measures are taken to curb this, then rapid ageing may increase the economic burden of chronic diseases by 40% by 2030 [4]. Furthermore, the burden of chronic diseases is not only heavy for countries, but also for individuals and households. For example, evidence from Iran showed that households with members suffering from chronic illnesses are more likely to experience economic hardships and are at a heightened risk of falling into poverty compared to other families [5]. In Greece, the incidence of CHE among households with chronically ill members is significantly higher than in others [6]. Further, several studies in China have observed that households with chronic conditions bear greater financial risks than others, especially in sub-poverty level families [7].
Despite extensive studies focus on CHE among older adults with chronic disease patients and the association between multimorbidity and CHE, there are still some research gap that need to be further explored. Existing studies have predominantly focused on the financial burden of specific severe diseases, such as cancer [8,9,10,11]. Other studies also emphasized the impact of multimorbidity on CHE [12,13,14]. To date, few studies have analyzed the association between chronic disease conditions and CHE, and there is also a lack of exploration on the differences of the impact of single and multiple chronic diseases on CHE in order to figure out subgroup inequities. In addition, most existing studies are cross-sectional, and it is necessary to supplement prospective cohort study designs to enhance the explanatory power of research conclusions.
Therefore, this study aims to use a nationally representative dataset from 2013 to 2020 to explore the association between chronic disease and CHE among elderly in China, and analyse the differences of the risks of poverty due to single chronic diseases and multimorbidity. This study helps to supplement and improve existing research, and also provides reference for the government to carry out more precise intervention measures based on the different condition of chronic diseases to prevent the occurrence of CHE.
Methods
Data sources
This study utilizes longitudinal data from the China Health and Retirement Longitudinal Study (CHARLS), a nationally representative household survey. The survey covered 150 counties in 28 provinces across China, aiming to collect a high-quality nationally representative sample of Chinese residents aged 45 and older. A detailed description of the objectives and methods of CHARLS has been reported elsewhere [15].
For the purpose of this analysis, the study included data from four survey waves—2013, 2015, 2018, and 2020. The initial 2013 survey serves as the baseline for this study, with data from 2015, 2018, and 2020 used to construct a balanced panel dataset. In the initial 2013 cohort, the study applied specific inclusion and exclusion criteria to refine the sample for longitudinal tracking. Households were excluded if they did not include any members aged 60 years or older or lacked key data points. To further focus on the financial impact of health issues, the study included elderly households that did not report catastrophic health expenditures in 2013. These households were then tracked in the 2015, 2018, and 2020 waves, creating a panel dataset for the cohort and resulting in a final sample of 6,483 participants. Figure 1 illustrates the sample selection process across different survey waves, detailing both the attrition and inclusion at each stage (Fig. 1).

Paticipant selection flowchart

Incidence of CHE among Chinese elderly households. (A) CHE incidence in total sample. (B) CHE incidence in participants according to chronic disease condition
Dependent variable
Catastrophic Health Expenditure (CHE) is a critical metric used to evaluate the financial impact of out-of-pocket health care expenditures on household finances. CHE occurs when these expenditures exceed a predefined threshold, representing a significant financial burden on households. Based on the definitions of CHE provided by the World Health Organization (WHO) and the World Bank, as well as existing research on CHE, the threshold by the WHO in 2009 is the most widely used, which defined a household as incurring catastrophic health expenditures when out-of-pocket spending on health equalled or exceeded 40% of a household’s capacity to pay.
Consistent with most studies, we use household non-food expenditure as a proxy for a household’s capacity to pay [14, 16,17,18]. Healthcare expenditure refers to the total out-of-pocket costs for outpatient and inpatient care incurred by the participant and their spouse over the past year.If a surveyed household’s annual health spending crosses the threshold, the dependent variable is coded as 1, indicating the presence of catastrophic health expenditures. If it does not, it is coded as 0, indicating absence.
Independent variable
In CHARLS, participants were asked to report if they had been diagnosed with any of the following 14 chronic diseases by a healthcare professional: including hypertension, dyslipidemia, diabetes, cancer or malignant tumor, chronic lung diseases, liver diseases, heart attack, stroke, kidney diseases, stomach and other digestive diseases, emotional, nervous and psychiatric problems, memory-related diseases, arthritis and rheumatism, and asthma. The definition and types of chronic diseases are derived from the original CHARLS questionnaire.
The primary independent variable in this study is chronic disease status. This variable was defined as a multi-category variable with three groups: respondents who did not report any chronic diseases are categorized as “no chronic disease,” respondents who reported having one chronic condition are categorized as “single chronic disease”, and respondents who reported having two or more chronic conditions are categorized as “multimorbidity”.
Covariates
The following variables were considered as potential covariates in this study. Demographic information includes gender (male, female) and age (in years). Marital status was defined as a binary variable with two categories: living with a spouse and not living with a spouse. Living with a spouse includes being married or cohabiting, while not living with a spouse includes being single, divorced, or widowed. Educational attainment was categorized as primary or below middle school level, and secondary or higher. Hukou type and place of residence were categorized as urban or rural.Hukou type is obtained from the registration system based on place of birth and lineage, and is a special identifier in China.Health insurance coverage was categorized as a binary variable (yes/no). The type of health insurance coverage was further subdivided into three major types of basic medical insurance programs in China: basic medical insurance for urban employees, basic medical insurance for urban residents, and the new rural cooperative medical scheme.
Statistical analysis
In the preliminary analysis, the baseline characteristics of the study participants were descriptively summarized using numbers and percentages based on the occurrence of CHE, and statistical comparisons were performed using the chi-square test.
This study employs a mixed-effects logistic regression model with panel data to explore the longitudinal impact of chronic diseases on CHE, with results presented as odds ratios (OR) and 95% confidence intervals (CI). Three models are constructed hierarchically to account for potential confounders. Model 1 is the crude model with no adjustment for covariates; Model 2 adjusts for basic demographic characteristics of participants (age, gender, education attainment, marital status); and Model 3 further includes household characteristics and other factors ( hukou type, place of residence, and health insurance).
We further conducted subgroup analyses stratified by covariates, creating interaction terms between the covariates and chronic disease status, and included these in the fully adjusted mixed-effects logistic regression model. Additionally, the stratifying variables were removed from the model to explore whether the interactions were statistically significant.
Sensitivity analyses
We conducted two sensitivity analyses. First, considering the significant economic burden associated with cancer, we excluded participants with cancer and repeated the analysis using the fully adjusted model. Additionally, we performed sensitivity analyses based on three different thresholds for CHE as defined by the World Health Organization (WHO) and the World Bank. CHE was defined in different ways: if out-of-pocket healthcare expenditure reached or exceeded 10% and 25% of total household consumption expenditure, or 25% of non-food household consumption expenditure [17].
These analyses were conducted to test the robustness of the results.Data from the CHARLS questionnaire were processed and cleaned using R programming language, ensuring accurate and efficient handling of the dataset. The statistical analyses were performed using Stata17. A two-sided p-value of less than 0.05 was considered statistically significant for all tests.
Result
Characteristics of study participants
This section describes the baseline characteristics of the participants. The average age of the participants is 65.85 years, reflecting the aging cohort under study.In terms of basic demographic characteristics, the gender distribution was slightly skewed towards females, who constituted 52.49% of the sample. The majority of participants have a low level of education, primarily at the primary school level or below(79.19%).This educational distribution is critical as it correlates with other socioeconomic factors such as employment in agriculture and living conditions. Most households had a strong familial support structure, as evidenced by 85.26% of household members being married or cohabiting, which may influence health outcomes and care-seeking behaviours.
Regarding household characteristics and other socioeconomic factors, the majority of respondents held rural hukou type(76.10%) and resided in rural areas(61.73%). This status has impacted their access to healthcare services and insurance, potentially posing specific challenges in obtaining medical resources and financial support. The basic medical insurance coverage rate has reached 92.80%, nearing universal coverage.
Table 1 shows the baseline characteristics stratified by chronic disease status. Participants who were older, male, less educated, held urban hukou, resided in urban areas, and had health insurance were more likely to be diagnosed with chronic diseases (all p < 0.05). In our sample, no significant difference was found between marital status (living with a spouse or not) and chronic disease prevalence (p > 0.05).The analysis sample includes a total of 6,483 participants who did not have CHE at baseline.
Figure 2 illustrates the incidence of CHE across the three survey waves in 2015, 2018, and 2020, as well as its distribution based on chronic disease status. Among elderly individuals in China, the incidence of CHE was 12.25% in 2015, increased to 18.73% in 2018, and reached 14.62% in 2020. Elderly individuals with single chronic diseases or multimorbidity had higher CHE incidence rates compared to those without chronic diseases.
Longitudinal relationship between chronic diseases and catastrophic health expenditure
To examine the impact of chronic diseases on catastrophic health expenditure (CHE), this study categorizes chronic disease prevalence into single chronic diseases and multimorbidity. A mixed-effects logistic regression model using panel data is employed to explore the longitudinal impact of chronic diseases on CHE, with results presented as odds ratios (OR) and 95% confidence intervals (CI). Three models are applied hierarchically to address potential confounding factors. Model 1 is a crude model with no adjustments for covariates; Model 2 adjusts for participants’ basic demographic characteristics (age, gender, education attainment and marital status); Model 3 further includes household characteristics and other socioeconomic factors (hukou type, place of residence, and health insurance).
Table 2 reports the stepwise regression results. The study results indicate that in all three models, the occurrence of chronic diseases significantly increases the risk of catastrophic health expenditure, regardless of whether it involves a single chronic condition or multimorbidity. In the crude Model 1, both single chronic diseases(P < 0.001, 95% CI: 1.16–1.44) and multimorbidity(P < 0.001, 95% CI: 1.10–1.36) significantly influence the occurrence of CHE. The results remain similar in Model 2, which adjusts for a few covariates. In the fully adjusted Model 3, both single chronic diseases(P < 0.001, 95% CI: 1.22–1.52) and multimorbidity(P < 0.001, 95% CI: 1.18–1.47) continue to significantly increase the risk of CHE.
The results for other covariates show that age(P < 0.01), education level (p < 0.001), marital status (p < 0.001), hukou(p < 0.001), and residence (p < 0.001) are significantly associated with CHE. Age is an important factor influencing catastrophic health expenditure in elderly households, the older the age, the higher the risk of CHE. Higher education levels reduce the occurrence of CHE. Living with a spouse may increase the risk of CHE. Co-residing couples constitute a larger household unit, potentially leading to higher overall medical needs. Elderly couples living together may both face health challenges, increasing the likelihood of incurring substantial medical costs. Compared to urban elderly households, rural elderly households are more prone to experiencing CHE. Notably, our data analysis indicates that basic medical insurance has no significant impact on CHE, suggesting that the current basic medical insurance system is insufficient to mitigate the risk of CHE for households. These findings highlight the substantial financial burden that chronic health conditions and other adverse circumstances can impose on families.
Detailed statistical results are presented in Table 2, illustrating the longitudinal impact of various variables on the likelihood of CHE occurrence within the cohort.
Stratification Analyses.
Stratification analysis
We further conducted stratified analyses to examine whether the impact of chronic diseases on catastrophic health expenditure (CHE) varies across different demographic subgroups, as illustrated in Fig. 3 The forest plot indicates that, after adjusting for covariates such as key demographic characteristics, the presence of chronic diseases is associated with a higher likelihood of CHE. This pattern of effect was consistently observed across various subgroups, including those defined by gender, education level, marital status, hukou type, place of residence, and health insurance. Furthermore, the interaction terms between the aforementioned covariates and chronic disease status were not statistically significant (all p-values for interaction > 0.05).
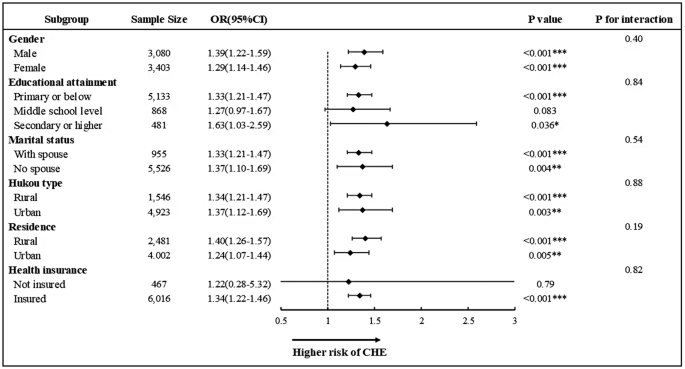
Association between chronic diseases and CHE across different subgroups. The forest plot depicts the longitudinal association between chronic diseases conditions and CHE across different covariate subgroups. All models were adjusted for a predefined full list of covariates (including age, gender, education, marital status, hukou type, place of residence and health insurance) except the stratification variable. (*p < 0.05, **p < 0.01, ***p < 0.001; 0R, odds ratio; CI, confidence interval)
Sensitivity analysis
To ensure the robustness of our findings, sensitivity analyses were conducted using two methods. First, considering the heavy economic burden imposed by cancer, we excluded participants diagnosed with cancer and repeated the above analysis using a fully adjusted model. The results, as shown in Table 3, indicate that after excluding cancer patients, chronic disease prevalence still significantly impacts catastrophic health expenditure.
The second sensitivity analysis was conducted by classifying catastrophic health expenditure using different thresholds.According to the definitions provided by the WHO and the World Bank, catastrophic health expenditure is defined in three ways: if out-of-pocket (OOP) healthcare expenditure equals or exceeds 10% and 25% of total household consumption expenditure, and 25% of total non-food household consumption expenditure. The consistency of results across these varying thresholds confirms the reliability of our main findings and suggests that our conclusions about the impact of chronic diseases on CHE are stable regardless of the specific threshold applied.
Additionally, through sensitivity analyses using different thresholds, we found that when CHE was defined as equal to or exceeding 40% of total non-food household consumption expenditure—a relatively high threshold—the likelihood of experiencing CHE increased by 36% and 32% for households with single chronic conditions and those with multiple chronic conditions, respectively, compared to households without chronic conditions. Notably, the impact of a single chronic condition on CHE surpassed that of multiple chronic conditions under this higher threshold. However, when applying the other three lower thresholds, the economic burden became more pronounced for households with multiple chronic conditions.
The outcomes of these sensitivity analyses are documented comprehensively in Table 4, providing a transparent view of how varying definitions of CHE affect the analysis.
Discussion
To our knowledge, this is the first study to utilize cohort data constructed from China’s latest nationally representative database of middle-aged and elderly individuals, employing cohort analysis to evaluate the longitudinal association between the prevalence of various chronic diseases and catastrophic health expenditure. Our study defines CHE as out-of-pocket medical expenses exceeding 40% of a household’s total non-food expenditure. Under this threshold, among households that had not experienced CHE in 2013, the incidence of CHE increased to 12.25% in 2015, 18.73% in 2018, and 14.62% in 2020, showing an overall upward trend consistent with findings from other studies. Compared to households without chronic diseases, households with one chronic disease and those with multiple chronic diseases exhibited significantly higher rates and severity of CHE, highlighting the profound impact of chronic diseases on household economic vulnerability. This study yields several important findings.
Previous studies on the prevalence of chronic diseases and household economic status have primarily focused on the comorbidity of chronic conditions, exploring the association between an increasing number of chronic diseases and rising healthcare expenditures [18, 19]. Several studies have focused on the impact of multimorbidity on CHE, identifying multimorbidity as a significant determinant of CHE [12, 14, 20,21,22,23]. In addition, some studies have focused on more severe conditions classified as chronic diseases, such as cancer, stroke, and heart disease, defining these conditions as “health shocks.” These studies suggest that such severe diseases, referred to as “health shocks,” are significant contributors to CHE [11,12,13,14,15]. However, our analysis reveals that even when only one household member suffers from a chronic disease—regardless of whether the disease falls under the category of severe conditions mentioned above—it can significantly impact the household’s economic situation, increasing the risk of poverty. This poses a substantial challenge to the healthcare expenditures, consumption levels, and living conditions of elderly households in China.
Furthermore, regarding the impact of different chronic disease statuses on CHE, our study found that although both single chronic diseases and multimorbidity significantly affect household economics, their risk characteristics differ. Using a higher CHE threshold—defined as equal to or exceeding 40% of total non-food household consumption expenditure—single chronic diseases may exert a more severe economic impact on households compared to multimorbidity.However, when the CHE thresholds are lowered to equal to or exceeding 10% or 25% of total household consumption, or 25% of non-food household consumption, multimorbidity poses a greater economic burden on households than single chronic diseases. This can be attributed to several reasons. First, as the CHE threshold decreases, more households may be able to absorb a portion of healthcare expenses without falling into catastrophic health expenditure. However, with the increase in the number of chronic conditions, household health expenditures rise correspondingly. Particularly for households with multimorbidity, the medical needs become more complex and frequent. Families dealing with two or more chronic conditions face heightened health challenges, leading to higher medical expenses for the treatment and management of these conditions. Consequently, households with multimorbidity are more likely to meet the CHE criteria under lower expenditure thresholds.Second, at lower expenditure thresholds, other household expenses (such as housing and transportation) account for a larger proportion of total consumption, reducing the share available for healthcare expenditures. This disproportionately affects households with multimorbidity, as they often require significantly more resources to address their health needs. Therefore, as the threshold decreases, the relative pressure of healthcare expenditures becomes more pronounced for households with an increasing number of chronic conditions.
This study also demonstrates that the relationship between chronic diseases and CHE remains consistent regardless of differences in gender, marital status, educational attainment, household registration type, place of residence, and health insurance coverage. A previous study that focused solely on multiple chronic diseases and CHE found similar results to those of this research, demonstrating that the impact of multimorbidity on CHE persisted across different household economic levels and all health insurance programs [14].
Social health insurance programs, organized and funded by the government, are intended to protect members from CHE. However, our findings indicate that China’s basic medical insurance has not significantly reduced the risk of CHE. This finding aligns with the results of earlier studies [19, 23,24,25,26,27]. Some studies have also highlighted that, even after the reforms, China’s medical insurance system failed to reduce the incidence of CHE [26,27,28,29,30,31]. The inefficiency of China’s health insurance system indicates that existing policies have failed to effectively alleviate the economic burden of chronic diseases on elderly households. This may be attributed to the high prevalence of chronic diseases among the elderly population and the limitations in the design and implementation of current policies. Despite the high medical costs in China, the actual reimbursement rates under basic medical insurance remain low, and the scope of coverage is limited. To address the issues mentioned above, this study proposes the following recommendations: First, expand the reimbursement scope and limits for chronic disease insurance, and adjust reasonable expenses based on disease progression to better support households with severe illnesses. Second, establish income-based deductibles to reduce the medical burden on elderly households and lower the risk of catastrophic health expenditure. Finally, optimize healthcare resource allocation, improve primary healthcare services, and reduce medical costs for residents.
However, several limitations of this study should be acknowledged. First, information on chronic disease prevalence was collected through self-reports, which may introduce recall bias into the results. Second, the estimation of CHE in our study is influenced by the questionnaire structure, data collection methods, and recall bias. Nevertheless, these limitations do not invalidate our findings, and the nature of large samples and the use of panel data helps to reduce estimation bias to some extent.
Conclusion
This study underscores the substantial impact of chronic illnesses on the risk of CHE among elderly households in China. Distinct from previous research, which predominantly concentrated on the economic implications of multiple comorbidities, this study provides groundbreaking evidence that even a single chronic illness can significantly impair a household’s financial stability, thereby markedly increasing the likelihood of CHE. Furthermore, this effect remains consistent across various socioeconomic dimensions, including gender, educational attainment, marital status, household registration, place of residence, and health insurance coverage.
Unexpectedly, despite the extensive coverage provided by existing social health insurance schemes, these programs have proven insufficient in effectively mitigating the risk of CHE. The findings of this study call for a comprehensive reassessment and recalibration of health and social policies to better safeguard elderly populations from the devastating financial consequences of catastrophic health expenditures. Addressing these critical issues will enable policymakers to design a more equitable and sustainable healthcare system that adequately meets the needs of China’s rapidly aging society.
Data availability
Publicly available datasets were analyzed in this study. This data can be found here: http://charls.pku.edu.cn/.
Abbreviations
- CHARLS:
-
China Health and Retirement Longitudinal Study
- CHE:
-
Catastrophic health expenditures
- SD:
-
Standard deviation
- CI:
-
Confidence interval
- OR:
-
Odds ratio
References
Van Damme W, Meessen B, Por I, Kober K. Catastrophic health expenditure. Lancet. 2003;362:996.
Kang J-H, Kim C-W. Relationship between Catastrophic Health expenditures and Income Quintile decline. Osong Public Health Res Perspect. 2018;9:73–80.
Peng W, Chen S, Chen X, Ma Y, Wang T, Sun X, et al. Trends in major non-communicable diseases and related risk factors in China 2002–2019: an analysis of nationally representative survey data. Lancet Reg Health - West Pac. 2024;43:100809.
Li X, Chen M, Wang Z, Si L. Forgone care among middle aged and elderly with chronic diseases in China: evidence from the China Health and Retirement Longitudinal Study Baseline Survey. BMJ Open. 2018;8:e019901.
Doshmangir L, Yousefi M, Hasanpoor E, Eshtiagh B, Haghparast-Bidgoli H. Determinants of catastrophic health expenditures in Iran: a systematic review and meta-analysis. Cost Eff Resour Alloc. 2020;18:17.
Skroumpelos A, Pavi E, Pasaloglou S, Kyriopoulos J. Catastrophic Health Expenditures and Chronic Condition Patients in Greece. Value Health. 2014;17:A501–2.
Miao W, Zhang X, Shi B, Tian W, Wu B, Lai Y, et al. Multi-dimensional vulnerability analysis on catastrophic health expenditure among middle-aged and older adults with chronic diseases in China. BMC Med Res Methodol. 2022;22:151.
Albright BB, Nitecki R, Chino F, Chino JP, Havrilesky LJ, Aviki EM, et al. Catastrophic health expenditures, insurance churn, and nonemployment among gynecologic cancer patients in the United States. Am J Obstet Gynecol. 2022;226:e3841–38413.
Incidence of household catastrophic. and impoverishing health expenditures among patients with Breast Cancer in Iran - PubMed. https://pubmed.ncbi.nlm.nih.gov/33836724/. Accessed 29 Jul 2024.
Private health insurance. and catastrophic health expenditures of households with cancer patients in South Korea - PubMed. https://pubmed.ncbi.nlm.nih.gov/29888826/. Accessed 29 Jul 2024.
Leng A, Jing J, Nicholas S, Wang J. Catastrophic health expenditure of cancer patients at the end-of-life: a retrospective observational study in China. BMC Palliat Care. 2019;18:43.
Tang S, Yao L, Li Z, Yang T, Liu M, Gong Y, et al. How do intergenerational economic support, emotional support and Multimorbidity affect the Catastrophic Health expenditures of Middle-aged and Elderly families?-Evidence from CHARLS2018. Front Public Health. 2022;10:872974.
Hong Y-R, Xie Z, Suk R, Tabriz AA, Turner K, Qiu P. Analysis of US Household Catastrophic Health Care expenditures Associated with Chronic Disease, 2008–2018. JAMA Netw Open. 2022;5:e2214923.
Zhao Y, Atun R, Oldenburg B, McPake B, Tang S, Mercer SW, et al. Physical multimorbidity, health service use, and catastrophic health expenditure by socioeconomic groups in China: an analysis of population-based panel data. Lancet Glob Health. 2020;8:e840–9.
Zhao Y, Hu Y, Smith JP, Strauss J, Yang G. Cohort profile: the China Health and Retirement Longitudinal Study (CHARLS). Int J Epidemiol. 2014;43:61–8.
Xu K, Evans DB, Kawabata K, Zeramdini R, Klavus J, Murray CJL. Household catastrophic health expenditure: a multicountry analysis. Lancet Lond Engl. 2003;362:111–7.
Cylus J, Thomson S, Evetovits T. Catastrophic health spending in Europe: equity and policy implications of different calculation methods. Bull World Health Organ. 2018;96:599–609.
Li H, Chen J, Su D, Xu X, He R. Is co-occurrence of Frailty and Multimorbidity Associated with increased risk of Catastrophic Health expenditure? A prospective cohort analysis in China. Risk Manag Healthc Policy. 2023;16:357–68.
Lee JT, Hamid F, Pati S, Atun R, Millett C. Impact of Noncommunicable Disease Multimorbidity on Healthcare Utilisation and Out-Of-Pocket expenditures in Middle-Income countries: Cross Sectional Analysis. PLoS ONE. 2015;10:e0127199.
Pati S, Agrawal S, Swain S, Lee JT, Vellakkal S, Hussain MA, et al. Non communicable disease multimorbidity and associated health care utilization and expenditures in India: cross-sectional study. BMC Health Serv Res. 2014;14:451.
Li H, Chang E, Zheng W, Liu B, Xu J, Gu W, et al. Multimorbidity and catastrophic health expenditure: evidence from the China Health and Retirement Longitudinal Study. Front Public Health. 2022;10:1043189.
Fu Y, Chen M, Si L. Multimorbidity and catastrophic health expenditure among patients with diabetes in China: a nationwide population-based study. BMJ Glob Health. 2022;7:e007714.
Zhai X, Zhang Q, Li X, Zhao X. Association between multimorbidity patterns and catastrophic health expenditure among Chinese older adults living alone. Arch Gerontol Geriatr. 2023;106:104892.
Zhao Y, Zhang P, Oldenburg B, Hall T, Lu S, Haregu TN, et al. The impact of mental and physical multimorbidity on healthcare utilization and health spending in China: a nationwide longitudinal population-based study. Int J Geriatr Psychiatry. 2021;36:500–10.
Kazibwe J, Tran PB, Annerstedt KS. The household financial burden of non-communicable diseases in low- and middle-income countries: a systematic review. Health Res Policy Syst. 2021;19:96.
Li Y, Wu Q, Xu L, Legge D, Hao Y, Gao L, et al. Factors affecting catastrophic health expenditure and impoverishment from medical expenses in China: policy implications of universal health insurance. Bull World Health Organ. 2012;90:664–71.
Liang X, Guo H, Jin C, Peng X, Zhang X. The effect of new cooperative medical scheme on health outcomes and alleviating catastrophic health expenditure in China: a systematic review. PLoS ONE. 2012;7:e40850.
Wagstaff A, Lindelow M. Can insurance increase financial risk? The curious case of health insurance in China. J Health Econ. 2008;27:990–1005.
Liu S, Coyte PC, Fu M, Zhang Q. Measurement and determinants of catastrophic health expenditure among elderly households in China using longitudinal data from the CHARLS. Int J Equity Health. 2021;20:62.
Li Y, Wu Q, Liu C, Kang Z, Xie X, Yin H, et al. Catastrophic health expenditure and rural household impoverishment in China: what role does the new cooperative health insurance scheme play? PLoS ONE. 2014;9:e93253.
Wang J, Zhu H, Liu H, Wu K, Zhang X, Zhao M, et al. Can the reform of integrating health insurance reduce inequity in catastrophic health expenditure? Evidence from China. Int J Equity Health. 2020;19:49.
Acknowledgements
We express our sincere gratitude to China Health and Retirement Longitudinal Study (CHARLS). Thanks to all authors who contributed to this study.
Funding
This study was supported by the National Natural Science Foundation of China Youth Fund Project (No. 72204048) and Shanghai Philosophy and Social Science Planning Projects (2023EGL002).
Author information
Authors and Affiliations
Contributions
XY conceived and designed the study, performed the data analysis, and wrote the original draft. DW assisted with data processing and statistical analysis.TZ provided revisions to the manuscript and raised constructive questions to optimize this study.QW refined the study design, oversaw the study implementation and analysis, and revised the manuscript. All authors read and approved the final version of the manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The studies involving human participants were reviewed and approved by the Biomedical Ethics Review Committee of Peking University (IRB0000105IRB00001052–11015). The patients/participants provided their written informed consent to participate in this study.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Yao, X., Wang, D., Zhang, T. et al. Chronic diseases and catastrophic health expenditures in elderly Chinese households: a cohort study. BMC Geriatr 25, 272 (2025). https://doiorg.publicaciones.saludcastillayleon.es/10.1186/s12877-025-05692-4
Received:
Accepted:
Published:
DOI: https://doiorg.publicaciones.saludcastillayleon.es/10.1186/s12877-025-05692-4